
University Of Cambridge’s Trial Successful For Use By Type 2 Diabetes Patients
Cambridge scientists have successfully trialled an artificial pancreas for use by patients living with type 2 diabetes. The device – powered by an algorithm developed at the University of Cambridge – doubled the amount of time patients were in the target range for glucose compared to standard treatment and halved the time spent experiencing high glucose levels.
Many people with type 2 diabetes struggle to manage their blood sugar levels using the currently available treatments, such as insulin injections. The artificial pancreas can provide a safe and effective approach to help them
Charlotte Boughton
Around 415 million people worldwide are estimated to be living with type 2 diabetes, which costs around $760 billion in annual global health expenditure. According to Diabetes UK, in the UK alone, more than 4.9million people have diabetes, of whom 90% have type 2 diabetes, and this is estimated to cost the NHS £10bn per year.
Type 2 diabetes causes levels of glucose – blood sugar – to become too high. Ordinarily, blood sugar levels are controlled by the release of insulin, but in type 2 diabetes insulin production is disrupted. Over time, this can cause serious problems including eye, kidney and nerve damage and heart disease.
The disease is usually managed through a combination of lifestyle changes – improved diet and more exercise, for example – and medication, with the aim of keeping glucose levels low.
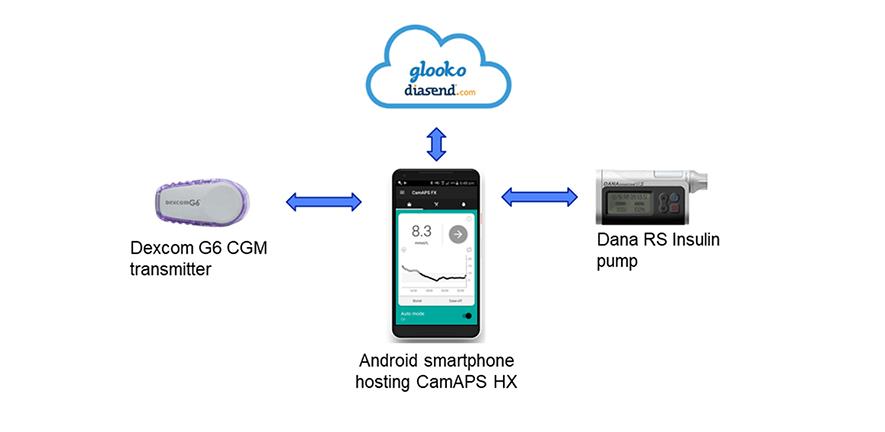
Researchers from the Wellcome-MRC Institute of Metabolic Science at the University of Cambridge have developed an artificial pancreas that can help maintain healthy glucose levels. The device combines an off-the-shelf glucose monitor and insulin pump with an app developed by the team, known as CamAPS HX. This app is run by an algorithm that predicts how much insulin is required to maintain glucose levels in the target range.
The researchers have previously shown that an artificial pancreas run by a similar algorithm is effective for patients living with type 1 diabetes, from adults through to very young children. They have also successfully trialled the device in patients with type 2 diabetes who require kidney dialysis.
Today, in Nature Medicine, the team report the first trial of the device in a wider population living with type 2 diabetes (not requiring kidney dialysis). Unlike the artificial pancreas used for type 1 diabetes, this new version is a fully closed loop system – whereas patients with type 1 diabetes need to tell their artificial pancreas that they are about to eat to allow adjustment of insulin, for example, with this version they can leave the device to function entirely automatically.
The researchers recruited 26 patients from the Wolfson Diabetes and Endocrine Clinic at Addenbrooke’s Hospital, part of Cambridge University Hospitals NHS Foundation Trust, and a local group of GP surgeries. Patients were randomly allocated to one of two groups – the first group would trial the artificial pancreas for eight weeks and then switch to the standard therapy of multiple daily insulin injections; the second group would take this control therapy first and then switch to the artificial pancreas after eight weeks.
The team used several measures to assess how effectively the artificial pancreas worked. The first was the proportion of time that patients spent with their glucose levels within a target range of between 3.9 and 10.0mmol/L. On average, patients using the artificial pancreas spent two-thirds (66%) of their time within the target range – double that while on the control (32%).
A second measure was the proportion of time spent with glucose levels above 10.0mmol/L. Over time, high glucose levels raise the risk of potentially serious complications. Patients taking the control therapy spent two-thirds (67%) of their time with high glucose levels – this was halved to 33% when using the artificial pancreas.
Average glucose levels fell – from 12.6mmol/L when taking the control therapy to 9.2mmol/L while using the artificial pancreas.
The app also reduced levels of a molecule known as glycated haemoglobin, or HbA1c. Glycated haemoglobin develops when haemoglobin, a protein within red blood cells that carries oxygen throughout the body, joins with glucose in the blood, becoming ‘glycated’. By measuring HbA1c, clinicians are able to get an overall picture of what a person’s average blood sugar levels have been over a period of weeks or months. For people with diabetes, the higher the HbA1c, the greater the risk of developing diabetes-related complications. After the control therapy, average HbA1c levels were 8.7%, while after using the artificial pancreas they were 7.3%.
No patients experienced dangerously-low blood sugar levels (hypoglycaemia) during the study. One patient was admitted to hospital while using the artificial pancreas, due to an abscess at the site of the pump cannula.
Dr Charlotte Boughton from the Wellcome-MRC Institute of Metabolic Science at the University of Cambridge, who co-led the study, said: “Many people with type 2 diabetes struggle to manage their blood sugar levels using the currently available treatments, such as insulin injections. The artificial pancreas can provide a safe and effective approach to help them, and the technology is simple to use and can be implemented safely at home.”
Dr Aideen Daly, also from the Wellcome-MRC Institute of Metabolic Science, said: “One of the barriers to widespread use of insulin therapy has been concern over the risk of severe ‘hypos’ – dangerously low blood sugar levels. But we found that no patients on our trial experienced these and patients spent very little time with blood sugar levels lower than the target levels.”
Feedback from participants suggested that participants were happy to have their glucose levels controlled automatically by the system, and nine out of ten (89%) reported spending less time managing their diabetes overall. Users highlighted the elimination of the need for injections or fingerprick testing, and increased confidence in managing blood glucose as key benefits. Downsides included increased anxiety about the risk of hypoglycaemia, which the researchers say may reflect increased awareness and monitoring of glucose levels, and practical annoyances with wearing of devices.
The team now plan to carry out a much larger multicentre study to build on their findings and have submitted the device for regulatory approval with a view to making it commercially available for outpatients with type 2 diabetes.
The research was supported by the National Institute for Health and Care Research (NIHR) Cambridge Biomedical Research Centre.